Seafood Poisoning at Sea: What Sailors in the Pacific Northwest and Alaska Need to Know

If you sail the Salish Sea, the Inside Passage, or anywhere along the Alaskan coast, you eat what the water gives you. Steamer clams from a sandbar. Oysters off the half-shell at the dock. Dungeness crab from a pot on the way home. The occasional dinner of mahi or tuna picked up in the tropics. This is one of the great pleasures of small-boat life. It's also, quietly, the source of more medical evacuations than most cruisers realize.
How common is this, really? Serious seafood poisoning is not an everyday event. Commercial shellfish in the US is extensively tested, and the regulatory programs in Washington and Alaska are among the best in the world. But recreational harvesters don't have that safety net, and when these illnesses strike, they move fast and often strike far from definitive care. That's the gap this article is meant to fill.
Two quick notes before we dive in:
This article is technical by necessity. The syndromes are distinct, the treatments differ, and the stakes at sea are high enough that vague summaries don't serve you. We've kept it as navigable as possible — use the section headers to find what's relevant to your waters, and the Field Triage table as your quick reference.
One term you'll see throughout: biotoxin (also called a shellfish toxin). It refers to a poison produced by a living organism — in this case, microscopic algae or bacteria — that ends up concentrated in seafood. Unlike bacterial food poisoning from bad storage, you can't smell, taste, or cook these toxins away. That's what makes them different, and why they warrant their own field guide.
There is no Wilderness Medical Society clinical practice guideline for seafood poisoning — we checked. The WMS guideline roster covers pit viper envenomation, burns, drowning, altitude, frostbite, and a handful of others, but marine biotoxins remain a content gap. That's a real problem, because the syndromes are distinct, the treatments are different, and at sea you may have to make the call days before you get to definitive care.
The Short Version
PSP (saxitoxin) — the lethal one. Check closures before every harvest.
ASP (domoic acid) — the permanent one. Don't eat crab viscera when DA is elevated.
Vibrio — the common one. Cook your oysters in summer.
Scombroid — the dramatic one. Antihistamines fix it.
Ciguatera — the tropical one. Don't eat barracuda. Anywhere.
NSP, DSP, and pufferfish/TTX are covered below. Less common in PNW waters, but worth reading if you're transiting south or harvesting recreationally.
The long version is below. It's worth reading if you sail outside cell range.
The Big Eight (or so)
Seafood poisoning isn't one disease. It's a category that contains at least eight clinically distinct syndromes, caused by different toxins or organisms, treated differently, and carrying very different prognoses. It’s important to note: most years in Washington state, serious shellfish illness involves dozens of cases, not hundreds. PSP deaths in Alaska averaged fewer than one per decade over the last 30 years. These aren't everyday emergencies. But they happen without warning, often in remote anchorages, and they move fast. That's the case for knowing this before you need it.
The ones you'll encounter on a PNW or Alaska boat, in rough order of regional relevance:
Paralytic Shellfish Poisoning (PSP) — saxitoxin
Amnesic Shellfish Poisoning (ASP) — domoic acid
Vibrio infections — V. parahaemolyticus, V. vulnificus
Diarrhetic Shellfish Poisoning (DSP) — okadaic acid
Scombroid (histamine) poisoning — bacterial breakdown of dark-meat fish
Ciguatera fish poisoning (CFP) — relevant if you're sailing south
Neurotoxic Shellfish Poisoning (NSP) — Gulf of Mexico
Pufferfish (tetrodotoxin) — rare, but worth a mention
1. Paralytic Shellfish Poisoning (PSP) — The One That Kills People in Alaska

This is the one. If you take nothing else from this post, take this.
The toxin: Saxitoxin and its ~57 chemical relatives. Produced by Alexandrium catenella and related dinoflagellates (microscopic algae that produce biotoxins — naturally occurring poisons) during blooms. Heat-stable. Cooking does not destroy it.
The vectors: Filter-feeding bivalves — clams, mussels, oysters, scallops, geoducks, and cockles. The toxin concentrates in the shellfish's tissues during a bloom.
The Alaska problem (this matters): Butter clams (Saxidomus gigantea) can retain saxitoxin in their siphons and gut for one to two years after a bloom ends. A recent multi-community Alaska study (Harley et al., 2024–2025, Toxins) tested over 950 butter clams from 18 Alaskan villages — about two-thirds of samples exceeded the FDA action threshold of 80 µg saxitoxin-equivalent per 100 g. Toxin distribution was wildly uneven across tissues (2–29% in the siphon tip, up to 65% in the gut), so the old folk practice of "just take the siphons off and you'll be fine" is not safe. (Harley 2024, PubMed)
Clinical: Onset 30 minutes to 2 hours. Tingling around the lips, spreading to face and extremities. Numbness, weakness, ataxia (loss of coordination), ascending paralysis, and ultimately respiratory failure. The patient stays mentally clear as paralysis ascends — they know exactly what's happening. This is the cruel feature.
Historical case fatality: ~8–15%. With modern mechanical ventilation, dramatically lower — but only if you get to ventilation.
Treatment: Supportive. Mechanical ventilation if respiratory failure develops. Activated charcoal if ingestion was recent and the patient can still protect their airway. No antidote.
Alaska epidemiology: PSP is the leading cause of seafood-related death in Alaska. The Alaska Section of Epidemiology Bulletin 2022-05 documents 132 reports and 5 fatal cases from 1993 to 2021, with deaths in 1994, 1997, 2010, and 2020 — roughly one death every six years over that span. Kodiak and Southeast Alaska are the highest-incidence regions. (AK DOH Bulletin 2022-05) The foundational paper is Gessner & Middaugh (1995, Am J Epidemiol) — 54 outbreaks, 117 cases, 4 intubations, 29 medevacs from 1973–1992. (PubMed)
👉 Washington/Bellingham: The WA Department of Health Biotoxin Program is active. The Shellfish Safety Map shows current closures across the Salish Sea. There is a 24-hour hotline: 1-800-562-5632. Hood Canal, Admiralty Inlet, and Whatcom County beaches all see recurring closures.
The bottom line: Commercial shellfish in the US are tested. Recreationally harvested shellfish — the bag of clams you dug on a beach, the mussels you pulled off a piling, the oysters from a buddy — are not. Check the WA DOH map (or the Alaska Department of Environmental Conservation) before every harvest. Saxitoxin is colorless, odorless, and survives cooking.
2. Amnesic Shellfish Poisoning (ASP) — The One That Steals Memory
The toxin: Domoic acid, produced by Pseudo-nitzschia diatoms. A biotoxin that causes damage to hippocampal neurons — the area of the brain responsible for forming new memories.
The vectors: Mussels (the original PEI outbreak), razor clams (the Pacific NW recurring problem), and Dungeness crab viscera — the "crab butter" inside the body cavity. Not the muscle meat. The viscera concentrate the toxin.
Clinical: GI symptoms within 24 hours (vomiting, cramps, diarrhea), then neurologic within 48 hours — headache, confusion, disorientation, seizures, sometimes ophthalmoplegia (eye-muscle paralysis) and hemiparesis. Severe survivors carry permanent anterograde amnesia — they can remember the past but cannot form new long-term memories. There is no recovery from established memory loss.
Landmark cases:
1987 Prince Edward Island: 107 patients, 3 deaths. Survivors with severe permanent memory deficits documented by Teitelbaum et al. in NEJM. (Perl 1990 | Teitelbaum 1990)
1991 Monterey Bay / PNW: A Pseudo-nitzschia australis bloom killed brown pelicans and Brandt's cormorants; coincident razor clam contamination triggered the first WA/OR coast closures.
2015 West Coast coastwide bloom: The largest recorded domoic acid event in North America. Linked to "the Blob" warm-water anomaly. Cost the Dungeness crab fishery roughly $97.5M in lost revenue. (McCabe 2016)
The Dungeness crab rule (regional, practical): When domoic acid is elevated, the toxin concentrates in the viscera and hepatopancreas — the soft yellow-orange "crab butter" inside the body cavity, not the muscle meat. Standard practice on the WA/OR coasts:
Remove the viscera and rinse the body cavity thoroughly before cooking.
Discard the cooking water. Do not use crab broth for chowder or stock.
Eat only the muscle meat from legs, claws, and the picked body.
Washington and California do not allow commercial landings of crab during DA closures. Oregon does, but only after evisceration. For recreational harvest, the WDFW domoic acid page and the WA DOH map are your authorities.
FDA action levels: 20 ppm domoic acid in shellfish; 30 ppm in crab viscera.
Treatment: Supportive. Benzodiazepines for seizures. No antidote.
3. Vibrio — The Summer Oyster Problem
If PSP is the killer and ASP is the memory thief, Vibrio parahaemolyticus is the most common ER visit. This is a real and rising PNW problem.
The organism: Vibrio parahaemolyticus (Vp) is a marine bacterium that grows in warm water (above ~15°C). The warmer the water, the more Vp in the oysters. PNW summers — and a long-term warming trend — are pushing infection rates up.
Clinical (Vp gastroenteritis): Watery diarrhea (sometimes bloody), cramps, vomiting, low-grade fever. Onset 12–72 hours after eating raw or undercooked shellfish (almost always oysters in the PNW). Self-limited in most healthy adults in 2–5 days.
The Alaska story: A 2004 outbreak on a cruise ship affected 62 passengers — Prince William Sound oysters were the source. This pushed the documented Vp range about 1,000 km farther north than previously known. The mean water temperature first exceeded the 15°C Vp-growth threshold during the implicated harvest period. Textbook climate-driven foodborne disease. (McLaughlin 2005, NEJM)
The 1997 PNW outbreak: 209 illnesses across California, Oregon, Washington, and BC — the largest culture-confirmed Vp outbreak in North America at the time. (CDC MMWR 1998)
Vibrio vulnificus is the dangerous cousin. Primary septicemia from raw shellfish ingestion (~50% mortality) or necrotizing fasciitis from wound exposure to seawater (~15–17% mortality). High-risk groups: people with chronic liver disease (especially cirrhosis), hemochromatosis (iron overload), immunocompromise, end-stage renal disease, and diabetes.
Treatment (severe Vibrio): Doxycycline 100 mg twice daily plus ceftazidime 2 g IV every 8 hours per CDC. Aggressive surgical debridement for necrotizing fasciitis — time-to-OR is an independent mortality predictor.
Prevention:
Cook shellfish thoroughly. Boil oysters until shells open, then keep boiling 3–5 minutes more. Internal temperature 145°F.
Immunocompromised people should not eat raw shellfish. This includes anyone on chemo, anyone with liver disease, anyone over 65 with chronic illness.
Wound care matters in warm water. If you cut yourself on a barnacle in August in Hood Canal, irrigate immediately, clean aggressively, and watch the wound. If it's red, hot, and progressing within hours, that's an ER visit.
👉 Washington regulatory: WA has a Vibrio Control Plan (WAC 246-282-006) governing commercial harvest May 1–September 30, with time-to-temperature requirements that get stricter in higher-risk beds.
4. Diarrhetic Shellfish Poisoning (DSP) — The Newer PNW Problem
The toxin: Okadaic acid and dinophysistoxins, from Dinophysis dinoflagellates. Mechanism: inhibits protein phosphatases in intestinal cells, causing secretory diarrhea.
Clinical: 30 minutes to a few hours after ingestion — profuse watery diarrhea, nausea, vomiting, abdominal cramps. Resolves in 2–3 days. Rarely fatal.
Why it matters here: The first recognized US DSP case cluster was in 2011 in Sequim Bay, WA — a family of three, from blue mussels harvested at Sequim Bay State Park. Toxins were 2–10× the FDA guidance level. This triggered the first US shellfish recall for DSP and formalized WA's routine monitoring program from 2012 forward. (Lloyd 2013, Emerg Infect Dis | Trainer 2013, Mar Drugs)
👉 DSP is now monitored alongside PSP and ASP in WA. The WA DOH DSP page tracks closures.
Treatment: Supportive — rehydration.
5. Scombroid (Histamine) Poisoning — The One That Looks Like an Allergy
You're south, you eat a poorly-iced tuna steak at a marina restaurant, and within an hour your face is red, you have hives, your heart is pounding, and you feel awful. This is not an allergy.
The mechanism: Bacteria (mostly Morganella morganii) convert the amino acid histidine in dark-fleshed fish into histamine — a biotoxin that forms not from algae, but from bacterial breakdown of the fish itself. This happens when the fish sits above 4°C after catch. The histamine is heat-stable, so cooking, smoking, canning, and freezing don't fix it. Cadaverine and putrescine block the body's ability to break histamine down at the gut wall, amplifying the effect.
Implicated fish: Tuna (~76% of US outbreaks per CDC surveillance), mahi-mahi, mackerel, skipjack, bonito, albacore, marlin, bluefish, amberjack, sardines, anchovies.
Clinical: Onset 10 minutes to 2 hours. Facial and upper-trunk flushing (sunburned look), urticaria (hives), throbbing headache, palpitations, tachycardia, hypotension, GI upset, sometimes bronchospasm. Pathognomonic clue: a peppery, sharp, or metallic taste at first bite. If the fish tastes wrong, spit it out.
Treatment: H1 antihistamine (diphenhydramine 25–50 mg PO) plus an H2 blocker (famotidine 20 mg PO). IV fluids if hypotensive. Epinephrine only if true anaphylactic features develop (stridor, airway compromise, refractory hypotension). Corticosteroids not indicated.
Differential from true fish allergy: Scombroid happens to people with no history of fish allergy and resolves cleanly in 8–12 hours. True IgE-mediated fish allergy is reproducible across exposures. (Feng 2016)
Prevention: Chill your catch hard. Tuna, mahi, and bonito on ice within minutes of landing. Below 4°C from boat to plate.
6. Ciguatera Fish Poisoning (CFP) — The Tropical Wildcard
If you sail your boat south, this is your concern.
The toxin: Ciguatoxins (CTX) from benthic dinoflagellates (Gambierdiscus, Fukuyoa) — biotoxins that live on reef macroalgae and biomagnify up the food chain. Small herbivorous fish eat the algae, big predators eat the small fish, and the toxin concentrates in the apex predators.
Implicated fish: Barracuda (highest risk — banned commercially in much of the endemic zone), grouper, snapper, amberjack, moray eel, hogfish, and other large reef predators. Viscera, liver, and roe are the worst parts. Bigger and older fish carry more toxin.
Clinical: Biphasic.
GI phase (1–24 hours, usually 6–12): nausea, vomiting, diarrhea, abdominal cramps.
Neurologic phase (within 48 hours, can persist for weeks to months): perioral and distal paresthesias (tingling around the mouth, hands, feet), intense pruritus (itching), myalgias, weakness, bradycardia, hypotension, and the near-pathognomonic cold allodynia / temperature reversal — cold objects feel burning hot. Symptoms can relapse with subsequent exposure to alcohol, nuts, caffeine, fish, or exertion for months.
Climate angle: Historically tropical/subtropical (35°N to 35°S). Now expanding northward with warming sea-surface temperatures — documented cases as far north as North Carolina (2007), the Canary Islands, Madeira, and the western Mediterranean. (Tester 2010, Toxicon | Friedman 2017, Marine Drugs)
Treatment: Supportive. Mannitol has been used historically for severe neurologic symptoms (1 g/kg IV over 30–45 minutes), but the only RCT (Schnorf 2002, Neurology) found no benefit over saline. Many clinicians still use it within 24–48 hours of onset. For chronic neuropathic symptoms, gabapentin or pregabalin is first-line; amitriptyline is the alternative. No specific antidote.
Prevention:
Don't eat barracuda. Anywhere.
Avoid the viscera, liver, and roe of any large reef predator from endemic waters.
Tasteless, odorless, and heat-stable — no cooking method helps, and no consumer test reliably catches it.
Local knowledge is your best filter. Ask harbor locals which species and which reefs to avoid.
7. Neurotoxic Shellfish Poisoning (NSP) — Gulf Coast, Briefly
The toxin: Brevetoxins from Karenia brevis (the Florida red tide organism). Voltage-gated sodium channel activators — mechanistically the opposite of saxitoxin.
Clinical: GI symptoms plus mild paresthesias and temperature reversal — milder than ciguatera. Aerosolized brevetoxin on Florida red tide beaches causes conjunctival irritation and bronchospasm in asthmatics. No ingestion deaths documented. (Fleming 2007, Chest)
Geography: Gulf of Mexico (especially the west coast of Florida), occasionally SE US Atlantic. Not established in the PNW. Worth knowing for southern transits.
8. Pufferfish / Tetrodotoxin — Brief
Clinical: Minutes-onset ascending paralysis with preserved consciousness, leading to respiratory failure. Indistinguishable from severe PSP at the bedside — both block voltage-gated sodium channels.
Sources: Pufferfish (fugu), blue-ringed octopus, certain newts. US cases are almost all from illegally imported or mislabeled product. (CDC MMWR 2014)
PNW wildlife note: The rough-skinned newt (Taricha granulosa) — common in Pacific Northwest forests — carries the highest tetrodotoxin concentration measured in any animal. Don't eat them. The dog who picks one up gets very sick.
Treatment: Supportive. Early intubation. No antidote.
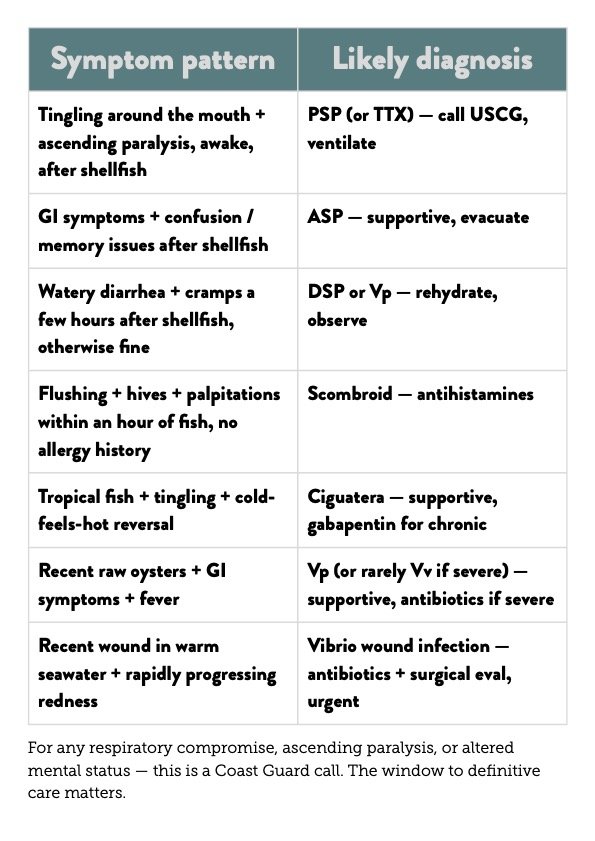
Field Triage: What to Do If Someone Gets Sick
Practical Prevention for a PNW/Alaska Boat
The boring stuff that works:
Check the WA DOH map or AK DEC closures before every recreational harvest. Saxitoxin and domoic acid are colorless, odorless, and survive every cooking method. There is no "smells fine" check.
Don't eat butter clams from areas with recent PSP closures, even months later. The siphon trick is unreliable.
Clean Dungeness crab the way WDFW guidance says — viscera out before cooking, body cavity rinsed, broth discarded.
Cook oysters thoroughly in summer. Especially if you're over 65, immunocompromised, or have liver disease.
Ice your catch hard. Tuna, mahi, and mackerel on ice in minutes, not hours.
Don't eat barracuda or large reef predators south of the line. Local knowledge wins.
Treat seawater wounds seriously in warm months. Especially Hood Canal and shallow PNW bays in July–September.
Carry the WA DOH biotoxin hotline in the boat's emergency contacts: 1-800-562-5632.
Final Takeaway
The PNW and Alaska are some of the best seafood waters on the planet — and some of the most monitored. The fatal cases are almost always recreational harvesters who didn't check closures, immunocompromised eaters who didn't cook their oysters, or cruisers who ate something they shouldn't have south of the line.
The math is straightforward:
PSP is the lethal one. Saxitoxin, butter clams, Alaska. Check closures, cook nothing into safety.
ASP is the permanent one. Domoic acid, razor clams and crab viscera. Don't eat the crab butter when DA is up.
Vp is the common one. Warm summer oysters, raw, immunocompromised eater. Cook them.
Scombroid is the dramatic one. Looks like an allergy, isn't.
Ciguatera is the tropical one. Don't eat barracuda. Anywhere.
There's no WMS clinical practice guideline for this. But the syndromes are well-described, the regional surveillance is excellent, and the prevention strategies are mostly free. Use the maps, watch your catch, and ice everything hard.
Selected References
WA / AK regulatory and surveillance
Washington Department of Health, Biotoxins Program: Shellfish Safety Map | Hotline 1-800-562-5632
WA DOH Vibrio Control Plan: doh.wa.gov
WA DOH DSP page: Diarrhetic Shellfish Poisoning
WDFW Domoic Acid in Crab: wdfw.wa.gov/fishing/basics/domoic-acid
Alaska Section of Epidemiology Bulletin 2022-05: Paralytic Shellfish Poisoning Update, 1993–2021
PSP
Gessner BD, Middaugh JP. Paralytic shellfish poisoning in Alaska: a 20-year retrospective. Am J Epidemiol. 1995;141(8):766-770. PubMed
Harley JR et al. Clam size explains some variability in PST in butter clams in Southeast Alaska. Toxins. 2024;16(11):464. PubMed
CDC. Paralytic Shellfish Poisoning — Southeast Alaska, May–June 2011. MMWR. 2011;60(45):1554. PubMed
ASP / domoic acid
Perl TM et al. Outbreak of toxic encephalopathy from mussels contaminated with domoic acid. N Engl J Med. 1990;322(25):1775-1780. PubMed
Teitelbaum JS et al. Neurologic sequelae of domoic acid intoxication. N Engl J Med. 1990;322(25):1781-1787. PubMed
McCabe RM et al. An unprecedented coastwide toxic algal bloom linked to anomalous ocean conditions. Geophys Res Lett. 2016;43(19):10366-10376. PMC
DSP
Lloyd JK et al. Diarrhetic shellfish poisoning, Washington, USA, 2011. Emerg Infect Dis. 2013;19(8):1314-1316. PubMed
Trainer VL et al. Diarrhetic shellfish toxins and other lipophilic toxins in Washington State. Mar Drugs. 2013;11(6):1815-1835. PubMed
Vibrio
McLaughlin JB et al. Outbreak of Vibrio parahaemolyticus gastroenteritis associated with Alaskan oysters. N Engl J Med. 2005;353(14):1463-1470. PubMed
CDC. Vibrio parahaemolyticus infections — Pacific Northwest, 1997. MMWR. 1998;47(22):457-462. PubMed
Bross MH et al. Vibrio vulnificus infection: diagnosis and treatment. Am Fam Physician. 2007;76(4):539-544. PubMed
Scombroid
Hungerford JM. Scombroid poisoning: a review. Toxicon. 2010;56(2):231-243. PubMed
Feng C, Teuber S, Gershwin ME. Histamine (Scombroid) Fish Poisoning: a Comprehensive Review. Clin Rev Allergy Immunol. 2016;50(1):64-69. PubMed
Ciguatera
Friedman MA et al. An Updated Review of Ciguatera Fish Poisoning: Clinical, Epidemiological, Environmental, and Public Health Management. Mar Drugs. 2017;15(3):72. PubMed
Tester PA et al. Ciguatera fish poisoning and sea surface temperatures in the Caribbean Sea and West Indies. Toxicon. 2010;56(5):698-710. PubMed
Schnorf H, Taurarii M, Cundy T. Ciguatera fish poisoning: a double-blind randomized trial of mannitol therapy. Neurology. 2002;58(6):873-880. PubMed
NSP / TTX
Fleming LE et al. Aerosolized red-tide toxins (brevetoxins) and asthma. Chest. 2007;131(1):187-194. PubMed
Cohen NJ et al. Tetrodotoxin poisoning from imported dried puffer fish. MMWR. 2014;63(51):1222-1225. PubMed
Maritime Medical Guides teaches Wilderness First Responder and Marine Medicine courses for offshore sailors, charter captains, and cruisers. We teach what the water does — including the parts the guidelines haven't caught up to yet.